Ensure healthy lives and promote well-being for all at all ages
Data extracted in April 2025.
Planned article update: June 2026.
Highlights

This article is a part of a set of statistical articles, which are based on the Eurostat publication ’Sustainable development in the European Union — Monitoring report on progress towards the SDGs in an EU context — 2025 edition’. This report is the ninth edition of Eurostat’s series of monitoring reports on sustainable development, which provide a quantitative assessment of progress of the EU towards the SDGs in an EU context.
SDG 3 aims to ensure health and promote well-being for all at all ages by improving reproductive, maternal and child health; ending epidemics of major communicable diseases; and reducing non-communicable and mental diseases. It also calls for reducing behavioural and environmental health risk factors.
Good health and well-being in the EU: overview and key trends
Health can be defined as ‘a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity’ [1]. Good health is not only of value to the individual as a major determinant of quality of life, well-being and social participation, it is also a basic precondition for general economic growth. Monitoring SDG 3 in an EU context focuses on the topics of healthy lives, determinants of health, causes of death and health care. Over the most recent five-year period assessed, developments regarding healthy lives and health care have largely been unfavourable, showing a stagnation in healthy life expectancy and a decline in self-perceived health combined with an increase in unmet need for medical care. Additionally, the consumption of antibiotics is not falling strongly enough for the EU to be on track to meet its respective 2030 target. Clear improvements have only been seen in the share of smokers, the rate of fatal work accidents and premature deaths due to air pollution. Other indicators on health determinants and causes of death have been stagnating or deteriorating over the most recent five-year period of available data.

Table 1: Indicators measuring progress towards SDG 3, EU
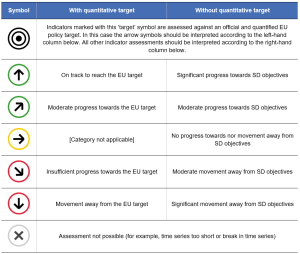
Table 2: Explanation of symbols for indicating progress towards SD objectives and targets


Healthy lives
The worldwide surge in life expectancy over the past century is a result of various factors, including reduced infant mortality, rising living standards, improved lifestyles and better education, as well as advances in health care and medicine.
Life expectancy has increased in EU countries over the past few decades, even though the pace of progress has temporarily slowed during the COVID‑19 pandemic [2]. While life expectancy gives an objective assessment of how long people can expect to live, it does not show whether people live their lives in good health. Thus, two indicators are included in the analysis. The first one, healthy life years at birth, shows the number of years a person can expect to live in a healthy state. The second one measures the share of people with good or very good perceived health, capturing an individual’s subjective view of their well-being.
Healthy life expectancy and self-perceived health of the EU population declined during the COVID-19 pandemic
In 2022, a child born in the EU could on average expect to live 62.6 years free from any severe or moderate disability. Women had a slightly higher healthy life expectancy, with 62.8 years, compared with 62.4 years for men. The overall EU figure masks considerable differences between Member States, with healthy life expectancy varying by 16.0 years between countries in 2022. Malta reported the highest number of healthy life years, with 70.2, followed by Italy with 67.4 and Greece with 67.0 years. In contrast, the lowest values were reported by Latvia and Denmark, with 54.2 and 55.9 years, respectively. Due to methodological changes in several Member States, the 2022 data are not comparable with data for earlier years. At EU level, a consistent time series is available for the period 2016 to 2021, which shows an overall slight decline in healthy life expectancy from 64.0 to 63.6 years. While there was an improvement between 2016 and 2019, healthy life expectancy fell by 1.0 years from 2019 and 2021 during the COVID-19 pandemic.
The decrease in overall life expectancy across the EU caused by the COVID-19 pandemic appears to have halted in 2022. While life expectancy at birth fell in 2020 and 2021 compared with the previous year, it increased by 0.5 years in 2022 and by a further 0.8 years in 2023. With 81.4 years in 2023, it slightly surpassed the pre-pandemic value of 81.3 years reported in 2019 [3].
The impact of the pandemic is also reflected in the data for self-perceived health. While the proportion of EU citizens rating their own health as good or very good increased between 2017 and 2020, it fell in 2021 and 2022. It increased again in 2023, reaching 67.9%. However, this is still 0.7 percentage points lower than in 2018. Similar to healthy life expectancy, this share varied strongly across Member States, ranging from 47.6% in Lithuania to 79.5% in Ireland and Malta. Furthermore, differences also exist between rural and urban areas. In 2023, the percentage of people who perceived their health to be good or very good was highest in cities (69.3%), slightly below the average in towns and suburbs (68.1%) and lowest in rural areas (65.4%) [4]. Moreover, the share of people with a disability — capturing a long-standing limitation to perform usual activities — who perceived their health as being good or very good was significantly lower than for the rest of the population. In 2023, 25.3% of people with a moderate disability and just 7.3% of people with severe disability perceived their health as being good or very good, compared to 85.0% of people without a disability [5].
Despite their higher healthy life expectancy at birth, women were less likely than men to rate their health as good or very good: 65.4% of women and 70.5% of men perceived their health as being good or very good in 2023 — a gap of 5.1 percentage points.
Health determinants
Many factors affect the health of individuals and populations. These include socio-economic factors, the state of the environment, city design, access to and use of health services, and individual characteristics and behaviour [6]. Lifestyle-related risk factors, such as an unhealthy diet, physical inactivity, smoking and excessive alcohol consumption, directly affect citizens’ quality of life and life expectancy. These factors also have a negative impact on the health and social systems of EU Member States, government budgets, and economic productivity and growth. The health determinants discussed in the following sections are obesity rate, smoking prevalence and noise pollution. In addition, further factors such as mobility and consumption patterns may also influence the health determinants described below.
More than half of the adult EU population is overweight
Obesity is a serious public health problem because it significantly increases the risk of chronic diseases, such as cardiovascular disease, type-2 diabetes, hypertension and certain types of cancer. For some individuals, obesity may also be linked to a wide range of psychological problems. From a societal perspective, obesity has substantial direct and indirect costs that put a considerable strain on health and social security systems. Furthermore, being obese or overweight from an early age can lead to more health problems in the long term [7].
In 2022, 14.8% of the EU population aged 18 or above were obese (with a body mass index equal to or greater than 30) and another 36.5% were pre-obese (with a body mass index between 25 and 30) [8]. In total, more than half of the EU population aged 18 or above were obese or pre-obese (and therefore overweight). Between 2017 and 2022, the share of both obese and pre-obese people decreased slightly by 0.1 and 0.4 percentage points, respectively. The total share of overweight people thus decreased slightly over this period, from 51.8% in 2017 to 51.3% in 2022.
The obesity rate generally increases with age, peaking at 65 to 74 years (19.7% obese in 2022) and decreasing again for people aged 75 and older. Young people aged 25 to 34 showed a lower obesity rate, at 9.7% in 2022. Moreover, obesity and pre-obesity rates decrease with higher educational levels, with 2022 obesity rates ranging from 10.5% for people with tertiary education to 17.9% for people with lower secondary education or lower [9]. In 2022, there was furthermore a considerable difference between Member States, with values ranging from 7.1% in Italy to 26.1% in Malta for obese people aged 18 and over.
Smoking prevalence among people aged 15 and over has decreased since 2009
Tobacco consumption is considered the single most preventable cause of illness and death worldwide. The World Health Organisation’s (WHO) European Region — that also includes some non-European countries such as Israel and some in Central Asia [10] — has one of the highest mortality rates attributable to tobacco use [11]. Tobacco use is the leading cause of 16% of all deaths among adults aged 30 years and over in Europe, which is above the global average of 12%. Many of these premature deaths result from multiple types of cancer and cardiovascular and respiratory diseases linked to tobacco use [12].
Smoking prevalence among the population aged 15 or over fell between 2009 and 2023, from 29% to 24%. In 2023, more men (28%) than women (21%) reported that they smoke. The age group with the highest prevalence of smokers were those aged 25 to 39 (32%) followed by those aged 44 to 55 (28%), younger people aged 15 to 24 years (22%) and older people aged 55 or over (19%). Lastly, the share of smokers who indicated they have trouble paying bills most of the time was higher than the share of smokers who said they (almost) never have trouble paying bills [13].
The number of people affected by noise from neighbours or the street is stagnating in the EU
Noise exposure reduces life satisfaction and perceived well-being. In addition, transport noise has been identified as the second most significant environmental cause of ill health in western Europe after air pollution [14]. The most harmful health problems — such as those affecting the cardiometabolic system — arise because of interrelated issues including decreased sleep quality and stress reactions in the human body. These issues can also lead to premature death [15]. In Europe, environmental noise is estimated to contribute to 12 000 premature deaths per year [16]. Road traffic is the dominant source of environmental noise, but railways, airports and industry also remain important sources of localised noise pollution [17]. The WHO Environmental Noise Guidelines for the European Region provide recommendations for protecting human health from exposure to environmental noise that originates from various sources.
In this publication, the perception of noise pollution is measured by the share of the population living in households who report they suffer from noise from neighbours or the street [18]. Since this measure is derived from subjective questions, a fall in the value of this indicator does not necessarily indicate a similar reduction in actual noise-pollution health effects that are instead calculated based on large-scale assessments and precise formulas derived by the WHO [19]. Since 2010, the share of the EU population feeling affected by noise from neighbours or the street has fallen slightly, from 20.6% in 2010 to 18.2% in 2023. However, since 2018 the share has stagnated. The perception of noise pollution is also unevenly distributed between Member States. In 2023, the proportion of people reporting noise disturbance from neighbours or the street ranged from 6.7% in Croatia to 31.3% in Malta.
Causes of death
Causes of death are among the oldest medical statistics available and play a key role in the general assessment of health in the EU. The data can be used to determine which preventive and medical curative measures or investment in research might increase a population’s life expectancy. The indicators selected for this sub-theme look at avoidable mortality, air pollution and fatal accidents on roads and at work.
Avoidable mortality fell again in 2022 after the COVID-19 related peak
Avoidable mortality refers to preventable and treatable causes of death, including injuries and drug-related diseases, as well as respiratory and infectious diseases, and some types of cancer. While avoidable mortality had been decreasing until 2019, the COVID-19 pandemic temporarily reversed the trend, resulting in strong increases in preventable deaths in 2020 and 2021. In 2022, avoidable mortality fell strongly after the 2021 peak, reaching 257.8 deaths per 100 000 persons in the age group below 75 years. Nevertheless, this value was 2.3% higher than five years earlier, with a rate of 252.1 in 2017, showing that avoidable mortality remained above pre-pandemic levels in 2022. This was mainly due to the developments in preventable mortality, which includes deaths by COVID-19 and which in 2022 was still 5.1% above the 2017 levels. In contrast, developments in treatable mortality were to a much lesser extent affected by the pandemic, and in 2022 deaths due to treatable causes were already 2.6% below the 2017 level. In 2022, COVID-19 remained among the top four causes of premature avoidable mortality, with a rate of 16.6 deaths per 100 000 persons, after ischaemic heart diseases (35.7 deaths per 100 000 persons), respiratory tract cancers (31.2) and stroke and other brain vessel diseases (18.4) [20]. Across Member States, the avoidable mortality rate in 2022 was lowest in Sweden, with 169.3 deaths per 100 000 persons aged less than 75 years, followed by Italy with a rate of 176.7 and Luxembourg with a rate of 180.2. In contrast, Latvia, Romania and Hungary reported the highest figures, with rates of 543.3, 519.3 and 511.8, respectively.
The number of premature deaths due to exposure to air pollution by fine particulate matter in the EU has decreased
According to the WHO, air pollution is the number one environmental cause of death in Europe [21]. It can lead to or aggravate many chronic and acute respiratory and cardiovascular diseases. Air pollution has been one of the EU’s main environmental policy concerns since the late 1970s. Air pollutants are emitted both naturally and as a result of human activities, with important sources being solid fuel combustion for domestic heating, industrial activities, road transport and agriculture. Urban populations are particularly exposed because of the daily flow of commuters, and the high concentration of industry and human activities causing the emission of fine particulate matter in EU cities. In addition, the most vulnerable citizens remain disproportionately affected by air pollution [22]. For example, groups with lower socioeconomic status tend to be disproportionately affected by air pollution because they often live closest to its source. Children are another disproportionally affected group because they have higher respiratory rates than adults, which increases their exposure to air pollution. Their developing immune systems and organs also make children more vulnerable to air pollution [23]. Air pollution also has a significant negative impact on the economy, by reducing both productivity and life expectancy, and by increasing health costs [24].
Fine particulate matter (PM2.5) is one of the most harmful components of air pollution for human health, causing an estimated 239 000 premature deaths in Europe in 2022. Between 2005 and 2022, premature deaths due to exposure to PM2.5 decreased by 44.6% [25]. This development suggests the EU is on track to meeting its target of reducing the negative impact of air pollution on health by 55% by 2030 compared with 2005, as set out in the Zero Pollution Action Plan (also see the Zero pollution monitoring and outlook 2025). According to an analysis by the European Environment Agency (EEA), if the trend seen in the past 17 years were to continue, the decline in the premature mortality attributable to PM2.5 would reach 63% by 2030 relative to 2005 levels.
Fatal work and road accidents have decreased, but further progress is necessary to meet the 2030 target of halving deaths from road crashes
Accidents were one of the most common causes of death within the EU in 2022, leading to almost 175 000 deaths or 3.4% of all deaths [26]. These accidents may happen at different places such as at home, leisure venues or work, as well as while travelling. Improving the working environment to protect employee health and safety is an important objective set out by the EU and its Member States in the Treaty on the Functioning of the European Union. Halving the number of deaths from road-traffic crashes is not only a global target, but also a goal of EU policies. The EU road safety policy framework 2021–2030 sets a target of reducing deaths and serious injuries by 50% by 2030 compared with 2019.
In 2023, 20 380 people were killed in road traffic crashes, equalling 4.5 deaths per 100 000 people. This represents a 12.6% reduction compared with 2018 and a 10.4% reduction compared with the reference year 2019, meaning the EU is still far from its 2030 target of halving the total death toll on EU roads relative to 2019. Nevertheless, the EU rate of 4.5 fatalities per 100 000 people compares favourably with the global average of around 15 per 100 000 [27]. Preliminary figures show that EU road fatalities fell to 19 800 deaths in 2024, a 3% improvement compared with 2023. Despite this positive step, the overall pace of improvement remains too slow. For further details see the article on SDG 11 ‘Sustainable cities and communities’.
Fatal accidents, leading to a person’s death within one year, may also occur at work. The EU made progress on this indicator between 2017 and 2022, reducing the number of fatal accidents at work per 100 000 employed persons from 1.79 to 1.66. There is a considerable difference between the sexes: the incidence rate for women (0.25) was negligible compared with the rate for men (2.9). This difference can be explained by the higher share of men working in occupations associated with a higher risk of work accidents. Non-fatal work accidents can also cause considerable harm, for example by leading to a permanent disability that may force people to leave the labour market or change their job. Non-fatal accidents happened considerably more often than fatal accidents, with an incidence rate of 1 507 per 100 000 employed persons in 2022 [28].
Health care
Access to health care — the timely access to affordable, preventive and curative health care — is high on the political agenda of EU countries. It is defined as a right in the Charter of Fundamental Rights and is one of the 20 principles of the European Pillar of Social Rights. Limited access to health care for some population groups, especially vulnerable populations, may result in poorer health outcomes and greater health inequalities. Reducing health inequalities is not only important for equity reasons, but also because it contributes to higher economic and social cohesion [29].
Unmet needs for medical care have increased since 2018
In 2023, 2.4% of the EU population aged 16 years or over reported an unmet need for medical care because of financial reasons, long waiting lists or travel distance. This represents a 0.6 percentage point increase since 2018, when the share was 1.8%. Differences in unmet needs for medical care remained substantial between Member States in 2023, ranging from 0.1% of the population in Malta and Cyprus to 12.9% in Estonia.
On average, 1.2% of the total EU population aged 16 years or over cited ‘waiting list’ as the most prominent reason for reporting an unmet need for medical examination in 2023. Furthermore, long waiting lists was the most common self-reported reason for unmet needs in cities and rural areas (1.3% each), which was slightly more than for people in towns or suburbs (1.0%). A further 1.0% of the total EU population reported financial constraints (‘too expensive’) as a reason for unmet needs for medical examination. This reason for unmet medical needs was more often declared in rural areas (1.3%) than in cities and towns and suburbs (1.0% each). However, not all Member States listed waiting lists as the main reason for unmet needs — in many countries costs were cited by most people [30].
Moreover, people with disabilities find it more difficult to access health care. In 2023, 6.2% of people with severe activity limitations and 4.5% of people with some activity limitations reported unmet needs for medical care due to the monitored reasons (financial, waiting list or distance), compared with only 1.4% of people without disabilities [31]. This discrepancy indicates that access to health care remains a challenge not only in certain parts of the EU but also for certain population groups.
Most European countries have achieved universal coverage for a core set of services, which usually include consultations with doctors, tests, examinations and hospital care. Yet in some countries, coverage of these services may not be universal or patients may have to bear the costs of accessing them. Furthermore, across the EU, around a seventh of all health spending was borne directly by households in 2022. Out-of-pocket payments as a share of total current health expenditure decreased slightly from 16.0% in 2014 to 14.3% in 2022. However, a considerable gap of 26.4 percentage points between countries remained in 2022. Moreover, households had to finance directly more than 30% of all spending in Malta, Lithuania, Latvia, Bulgaria and Greece. Meanwhile in Croatia, France and Luxembourg, the share of out-of-pocket spending was below 10% [32]. Poor households and those who have to pay for long-term treatment such as medicines for chronic illness are at high risk of experiencing financial hardship as a result of having to pay out of their own pockets.
Out-of-pocket payments can pose a serious problem for low-income households, because they prevent people from spending on other essential items such as food, housing and utilities (gas, electricity and water). The problem is particularly acute if it is combined with a reduction in financial resources for health care systems caused, for example, by an economic crisis. Private spending through voluntary health insurance (VHI) and out-of-pocket payments (OOPs) is sometimes seen as a way to make up for public shortfalls. However, private spending on health is far from a perfect substitute for public spending. Both OOPs and VHI can undermine equity of access by skewing the distribution of health spending in favour of richer people, sometimes at the expense of poorer, sicker and older people [33].
The total consumption of antibiotics in the EU has fallen, although there are substantial differences between Member States
Antimicrobial resistance (AMR) is a serious cross-border threat to health in the EU [34]. From 2016 to 2020, AMR led to more than 35 000 deaths in the EU/EEA each year [35]. Policies that tackle AMR with a ‘One-Health’ approach can save lives and healthcare costs. Antimicrobial consumption (AMC) is one of the main drivers of the development of AMR. This is aggravated by the inappropriate use of antimicrobials in humans, animals and plants. Reduction of AMC by using antimicrobials prudently and only where needed reduces selective pressures on the pathogens that contribute to the development of multi-drug resistance.
In humans, AMC is expressed as the number of defined daily doses (DDD) per 1 000 inhabitants per day, which provides an estimate of the proportion of the population treated daily with antimicrobials. In 2023, the EU population-weighted mean total AMC of antibacterials for systemic use (ATC group J01) in the community and hospital sectors was 20.0 DDD per 1 000 inhabitants per day, which is 7.6% lower than in 2013. In the short term, since 2018, the EU population-weighted mean total consumption of antibacterials for systemic use has decreased by 1.1%, indicating only slow progress towards the EU target to reduce the total consumption of antibiotics in humans by 20% by 2030 relative to 2019 [36]. Additionally, significant differences between Member States can be observed. In 2023, country-specific means ranged from 9.6 DDD per 1 000 inhabitants per day in the Netherlands to 28.5 in Greece.
Antimicrobial-resistant bacteria derived from food-producing animals can spread to humans by ingestion of or from handling food contaminated with zoonotic bacteria. Over time, this makes the antimicrobials less effective, resulting in treatment failure [37]. Thus, in addition to reducing human consumption of antimicrobials in the community and hospital sectors, the EU has set a target to reduce overall EU sales of antimicrobials for farmed animals and in aquaculture by 50% by 2030 relative to 2018. According to a 2025 report from the European Medicines Agency, the EU achieved a 25.2% reduction in sales of antimicrobials for farmed animals and in aquaculture by 2023 compared with the 2018 baseline. This is the result of declining sales in almost all Member States. While the EU is thus about halfway to the 2030 target, further declines in EU sales of antimicrobials are needed.
Main indicators
Healthy life years at birth

This indicator measures the number of years at birth that a person can expect to live in a healthy condition. Healthy life years is a health expectancy indicator which combines information on mortality and morbidity (prevalence of the population suffering from a disease or medical condition).
.png)
Note: y-axis does not start at 0.
Source: Eurostat (sdg_03_11)
.png)
People with good or very good self-perceived health

This indicator is a subjective measure of how people judge their health in general on a scale from ‘very good’ to ‘very bad’. The data stem from the EU Statistics on Income and Living Conditions (EU-SILC). Indicators of perceived general health have been found to be a good predictor of people’s future health care use and mortality.
.png)
Note: y-axis does not start at 0.
Source: Eurostat (sdg_03_20)
.png)
Source: Eurostat (sdg_03_20)
Smoking prevalence

This indicator measures the percentage of the population aged 15 years and over who report they currently smoke boxed cigarettes, cigars, cigarillos or a pipe. It does not include the use of other tobacco and related products such as electronic cigarettes and snuff. The data are collected through a Eurobarometer survey and are based on self-reported use during face-to-face interviews in people’s homes.
.png)
Note: y-axis does not start at 0.
Source: European Commission services, Eurostat (sdg_03_30)
.png)
Source: European Commission services, Eurostat (sdg_03_30)
Standardised avoidable mortality

Avoidable mortality covers both preventable and treatable causes of mortality. Preventable mortality refers to mortality that can mainly be avoided through effective public health and primary prevention interventions (carried out before the onset of diseases/injuries to reduce incidence). Treatable mortality can mainly be avoided through timely and effective health care interventions, including secondary prevention and treatment (after the onset of diseases to reduce case-fatality). The total avoidable mortality rate includes a number of infectious diseases, several types of cancers, endocrine and metabolic diseases, as well as some diseases of the nervous, circulatory, respiratory, digestive and genitourinary systems, some diseases related to pregnancy, childbirth and the perinatal period, a number of congenital malformations, adverse effects of medical and surgical care, a list of injuries and alcohol and drug-related disorders.
.png)
Source: Eurostat (sdg_03_42)
.png)
Source: Eurostat (sdg_03_42)
Self-reported unmet need for medical care

In the context of SDG monitoring, this indicator measures the share of the population aged 16 and over reporting unmet needs for medical care due to one of the following reasons: ‘financial reasons’, ‘waiting list’ and ‘too far to travel’. Self-reported unmet needs concern a person’s own assessment of whether they needed medical examination or treatment (dental care excluded) but did not have it or did not seek it. The data stem from the EU Statistics on Income and Living Conditions (EU-SILC). Since social norms and expectations may affect responses to questions about unmet care needs, caution is required when comparing differences in the reporting of unmet medical examination across countries. In addition, the different organisation of health care services is another factor to consider when analysing the data. Finally, there are also some variations in the survey questions across countries and across time [38].
.png)
Note: y-axis does not start at 0.
Source: Eurostat (sdg_03_60)
.png)
Source: Eurostat (sdg_03_60)
Consumption of antibiotics in the community and hospital sectors

This indicator measures the total antimicrobial consumption (AMC) in the community and hospital sectors. AMC is expressed as the number of defined daily doses (DDD) per 1 000 inhabitants per day. The data refer to the Anatomical Therapeutic Chemical (ATC) classification code J01 ‘Antibacterials for systemic use’. The data for the EU aggregate are presented as population-weighted mean and include imputations and adjustments [39].
_per_1_000_inhabitants_per_day).png)
Source: ESAC-Net, ECDC, Eurostat: (sdg_03_70)
_per_1_000_inhabitants_per_day).png)
Source: ESAC-Net, ECDC, Eurostat: (sdg_03_70)
Footnotes
- ↑ World Health Organization (1946), Constitution of the World Health Organization.
- ↑ Source: Eurostat (online data code: (demo_mlexpec)).
- ↑ Ibid.
- ↑ Source: Eurostat (online data code: (hlth_silc_18)).
- ↑ Source: Eurostat (online data code: (HLTH_DH010)).
- ↑ World Health Organization (2024), Social determinants of health.
- ↑ World Health Organization (2021), Obesity: New analysis from WHO/Europe identifies surprising trends in rates of overweight and obesity across the Region.
- ↑ The indicator measures the share of obese people based on their body mass index (BMI). BMI is defined as the weight in kilograms divided by the square of the height in metres. People aged 18 years or over are considered obese with a BMI equal to or greater than 30. Other categories are: underweight (BMI less than 18.5), normal weight (BMI between 18.5 and less than 25), and pre-obese (BMI between 25 and less than 30). The category overweight (BMI equal or greater than 25) combines the two categories pre-obese and obese.
- ↑ Source: Eurostat (online data code: (ilc_hch10)).
- ↑ The WHO European Region also includes some non-European countries such as Israel, Uzbekistan, Turkmenistan or Tajikistan; see https://www.who.int/countries for the full list of countries.
- ↑ World Health Organization (2012), WHO global report: mortality attributable to tobacco, p.14.
- ↑ World Health Organization (2024), WHO report on the global tobacco epidemic, 2023: Protect people from tobacco smoke.
- ↑ European Commission (2024), Attitudes of Europeans towards tobacco and electronic cigarettes, Special Eurobarometer 539.
- ↑ European Environment Agency (2018), Environmental noise.
- ↑ European Environment Agency (2021), Managing exposure to noise in Europe.
- ↑ European Environment Agency (2020), Healthy environment, healthy lives: how the environment influences health and well-being in Europe, Publications Office of the European Union, Luxembourg.
- ↑ European Environment Agency (2021), Managing exposure to noise in Europe.
- ↑ It needs to be noted that the figures on noise disturbance presented here include noise from neighbours and therefore go beyond the scope of the Environmental Noise Directive.
- ↑ Also see: European Environment Agency (2019), Environmental noise.
- ↑ Source: Eurostat (online data code: (hlth_cd_apr)).
- ↑ European Environment Agency (2024), Europe’s air quality status 2024.
- ↑ European Environment Agency (2018), Unequal exposure and unequal impacts: social vulnerability to air pollution, noise and extreme temperatures in Europe, Publications Office of the European Union, Luxembourg.
- ↑ Ibid.
- ↑ European Environment Agency (2022), Air quality in Europe 2022.
- ↑ European Environment Agency (2024), Harm to human health from air pollution in Europe: burden of disease status, 2024.
- ↑ Source: Eurostat (online data code: (hlth_cd_aro)).
- ↑ WHO (2023), Global status report on road safety 2023, Geneva.
- ↑ Source: Eurostat (online data code: (hsw_mi08)).
- ↑ European Council (2014), Council conclusions on the economic crisis and healthcare, 2014/C 217/02.
- ↑ Source: Eurostat (online data code: (HLTH_SILC_21)).
- ↑ Source: Eurostat (online data code: (hlth_dh030)).
- ↑ Source: Eurostat (online data code: (hlth_sha11_hf)).
- ↑ Expert Panel on effective ways of investing in health (EXPH) (2016), Access to health services in the European Union, final opinion approved at the 14th plenary meeting of 3 May 2016 after public consultation, p. 18.
- ↑ European Parliament and the Council of the European Union (2022), Regulation 2022/2371 on serious cross-border threats to health and repealing Decision No 1082/2013/EU.
- ↑ European Centre for Disease Prevention and Control (ECDC) (2022), Assessing the health burden of infections with antibiotic-resistant bacteria in the EU/EEA, 2016–2020, ECDC, Stockholm, pp. 4-7.
- ↑ Council of the European Union (2023), Council Recommendation on stepping up EU actions to combat antimicrobial resistance in a One Health approach, 2023/C 220/01.
- ↑ European Food Safety Authority (EFSA) and European Centre for Disease Prevention and Control (ECDC) (2023), The European Union Summary Report on Antimicrobial Resistance inzoonotic and indicator bacteria from humans, animals and food in 2020/2021. EFSA Journal 2023;21(3):7867.
- ↑ OECD/EU (2018), Health at a Glance: Europe 2018 — State of Health in the EU Cycle, OECD Publishing, Paris, p. 170.
- ↑ European Centre for Disease Prevention and Control (2023), Antimicrobial consumption in the EU/EEA (ESAC-Net) — Annual Epidemiological Report 2022, ECDC, Stockholm.
Explore further
Other articles
Database
Thematic section
Publications
Further reading on good health and well-being
- EEA (2025), Air quality status report 2025.
- EEA (2019), Healthy environment, healthy lives: how the environment influences health and well-being in Europe, European Environment Agency, Copenhagen.
- European Environment Agency & Joint Research Centre (2025), Zero pollution monitoring and outlook 2025, Publications Office of the European Union, Luxembourg.
- European Medicines Agency, Antimicrobial resistance in human medicine.
- OECD & European Commission (2024), Health at a Glance: Europe 2024, OECD Publishing, Paris.
- WHO (2019), Environmental Noise Guidelines for the European Region, WHO Regional Office for Europe, Copenhagen.
- World Health Organization (2023), WHO report on the global tobacco epidemic, 2023: Protect people from tobacco smoke.
Methodology
More detailed information on EU SDG indicators for monitoring of progress towards the UN Sustainable Development Goals (SDGs), such as indicator relevance, definitions, methodological notes, background and potential linkages can be found in the introduction as well as in Annex II of the publication ’Sustainable development in the European Union — Monitoring report on progress towards the SDGs in an EU context — 2025 edition’.
External links
Further data sources on good health and well-being
- ECDC, COVID-19.
- EEA, European zero pollution dashboards – Health.
- EEA, Health.
- European Medicines Agency, Antimicrobial Sales and Use Platform.
- World Bank, Atlas of Sustainable Development Goals.
- WHO (2024), World Health Statistics 2024: Monitoring health for the SDGs.